


Forensic Evidence From the Clotshot
I tested my COVID-jabbed patients for D-dimer, a breakdown product of clotting, a telltale sign of prior clotting activity. Each lab result came back high, even long after the last jab.

Warning against self-harm
I would guess that the Venn Diagram of people who chose to submit to COVID vaccines and those who rely primarily on naturopathic medicine for their healthcare have very little intersection. Skepticism of conventional medicine is robust among those who have seen undesirable pharmaceutical effects on themselves and loved ones. So this growing contingent tends to avoid conventional medicine, unless necessary, choosing instead chiropractic, naturopathic, acupuncturist, herbalist and homeopathic practitioners as primary providers.
However, there is still a small minority of seldom-consulting pharma-adherents in my practice, among both new patients to me and some whom I had not seen in years, since before COVID. In my case as a practicing naturopathic physician, there were twelve total people in my practice who had decided to submit to COVID vaccination before we consulted.
What happened to twelve COVID-vaccinated people
Unfortunately, a patient whom I had not seen in a while died suddenly and unexpectedly eleven days after his one COVID vaccine dose. Two others had been in remission from cancer after finishing our clinic’s treatments for 14 and 5 years respectively. The latter person’s cancer returned within a few months after the jab. Another never had cancer, but I had not seen him since before COVID, and he had felt bullied into getting two shots, not knowing that I write medical exemptions. I learned of those four people’s COVID shots during early to mid-2021. None of those four returned for care after COVID vaccines, nor for a D-dimer lab.
I consulted later with each of the remaining eight patients. Of those, I offered three new patients, as of early 2022, the D-dimer lab, and they declined. That leaves five remaining COVID vaccinated patients from mid-2022 on. Of those, I saw four returning patients whom I had not seen in years, since before COVID. I recommended to each of four, plus a very new patient, (subtotal five) that each get the D-dimer lab, so that we could have some idea about the impact of the COVID vaccines, and if it would be prudent to take any measures, and each of them agreed to have their blood drawn for this D-dimer lab.
So the following data is from those five patients. Notably, fibrinogen, PT/INR, platelets and troponin were all normal. Of those, only D-dimer was out of range.
Sam, Tim, Ann, Joe and Jen (all very different from their real names) are all from early 60’s to early 80’s in age. All five had at least one COVID vaccine. They are all certain that they did not have any COVID vaccine doses as late as Summer 2022. Most of the doses were during 2021, with a latest dose in early 2022. D-dimer labs were all drawn within the last quarter of 2022.
But first, an explanation of D-dimer
D-Dimer is a protein of two parts or "mer," hence dimer. D refers to dextrorotation, or a right-handed spiral structure. I ordered this lab, because D-dimer is a breakdown product from fibrin, so it's helpful for knowing if there has been excessive clotting going on. The presence of high D-dimer gives evidence that the body has been fighting (with some success) against one or more clots that have been held together by fibrin threads.
I have been asking my covid-jabbed patients (and from earlier, other cardiovascular history patients) if we may draw for this lab, because it lets me know if we need to keep an extra careful eye on blood viscosity, clotting time, risk for clots, and / or blood-thinning strategies. (Which all open a new can of worms, because homeostatic anti-coagulation is also going on, and neither excess bleeding nor clotting can be risked. So this is a whole other set of challenges for those who had the "clotshot.")
Now I admit that this is a very tiny retrospective case series. That said, it turns out that all but one of my patients who agreed to a D-dimer lab are coming back above normal range. Sam and Tim were roughly triple and quadruple, respectively, the top of normal range after two COVID vaccine doses each. Ann was at the 79th percentile of the more generous lab reference range. All five are way above range in the following Medscape range of < 250 ng/mL.
Medscape refers to the clinical reference Mosby’s Diagnostic & Laboratory Test Reference, 14th ed. Elsevier, 2019, by KD Pagana, TJ Pagana, et al, in which the D-dimer reference range is < 250 ng/mL.
From https://emedicine.medscape.com/article/2085111-overview
Here is the Medscape interpretation of D-dimer levels:
Unlike other markers for thrombotic tendency, high D-dimer can reflect a chronic tendency toward active fibrin formation and degradation, that is, the body’s tendency to clot excessively, as well as for homeostatic opposition to that tendency, leading to the (somewhat) successful disintegration of fibrin, aka clot-busting. (Interestingly, my COVID-vaccinated patients were all normal in all other clotting indicators and clues that we tested: platelets, fibrinogen, PT / INR and troponin, but all had concerning D-dimer levels. This suggests some successful homeostatic normalization that the most unfortunate “clotshot” victims have not been able to achieve.) D-dimer is often used as an indicator, along with lung imaging, of whether a deep vein thrombosis has developed into a pulmonary embolism. None of my five patients above had or developed a pulmonary embolism, although Jen did have a small DVT, now resolved.
Conditions that may be correlated with an elevated D-dimer include deep vein thrombosis, pulmonary embolism, acute stroke, aortic dissection or other vascular flow anomalies, traumatic brain injury and cancer.
D-Dimer Reference Ranges
D-dimer is considered normal in the US when below 500 ng/mL or 250 ng/mL. It turns out to be inversely correlated with longevity. In a four-year study of 17,359 apparently healthy, randomly recruited adults, > 35 years old, mean age 55, in southern Italy, reported in 2013 by Di Castelnuovo, de Curtis, et al, D-dimer showed no significant association with either age, sex, smoking, BMI, alcohol consumption, hypertension or diabetes. However, in accordance with smaller earlier studies, high D-dimer concentration in the blood was independently associated with higher rates of subsequent death from any cause. The risk was found to increase for D-dimer > 210 ng/mL.
From Di Castelnuovo et al Table 4, deaths from all causes skewed strongly toward the highest quartile of D-dimer results, although that was 8% of the study population; conversely, note the longevity association with low (< 221) D-dimer:
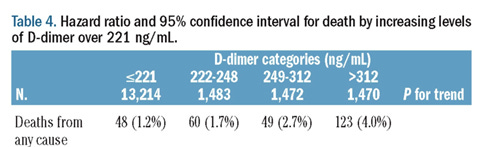
Here was the distribution of D-dimer levels, with hazard and C/I for each level.
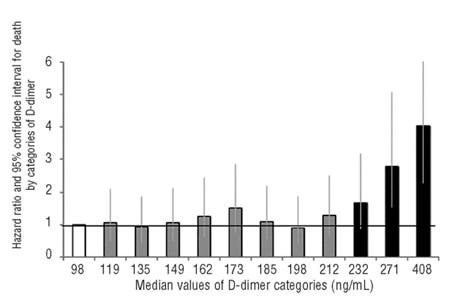
Let’s now plot the distribution of this Mediterranean adult pre-COVID population’s D-dimer levels against the levels we have found in our COVID era, COVID vaccinated patients:
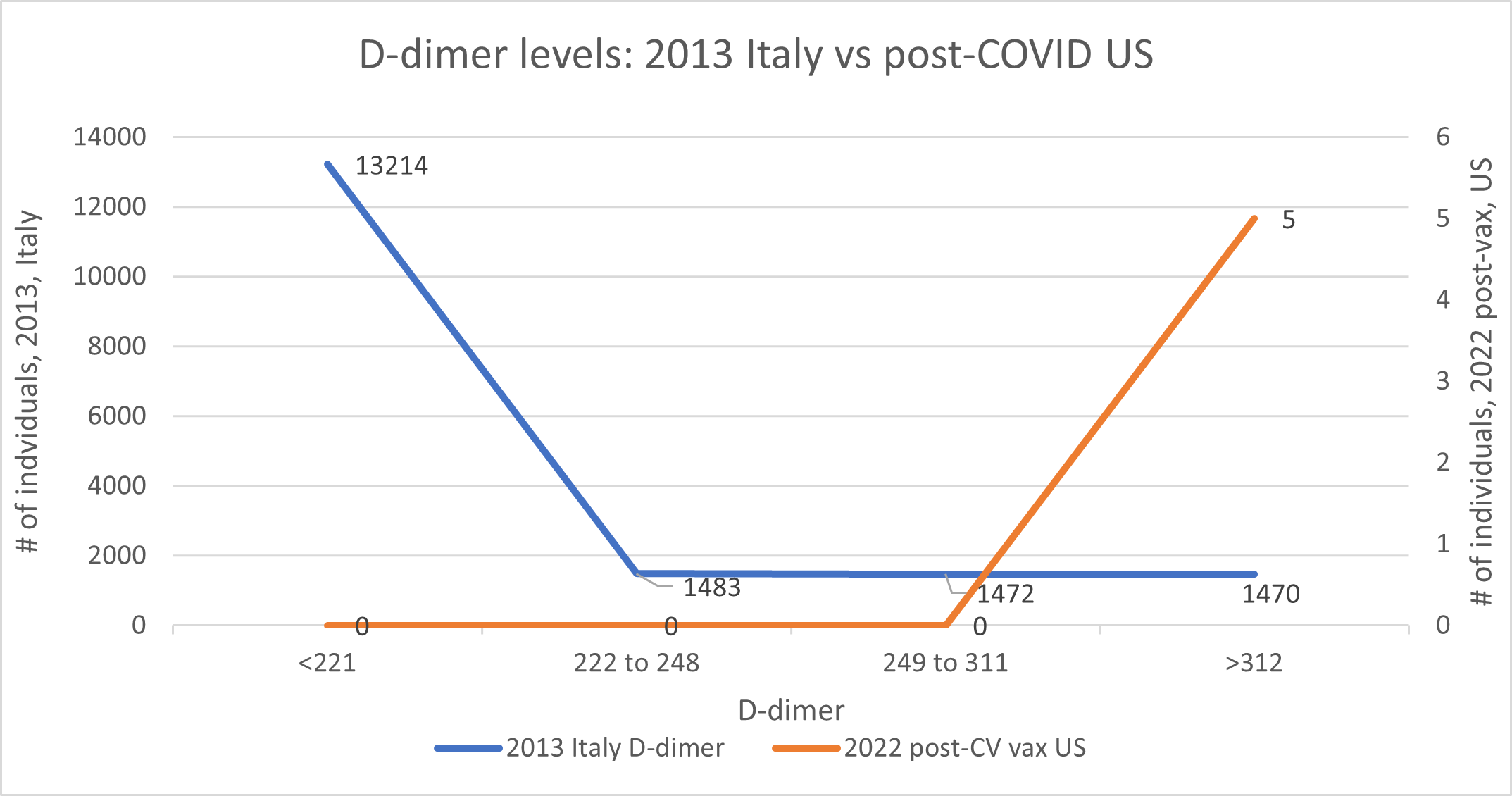
This distinction between the 2013 healthy adult Italian population and the five COVID-vaccinated US patients is quite stark.
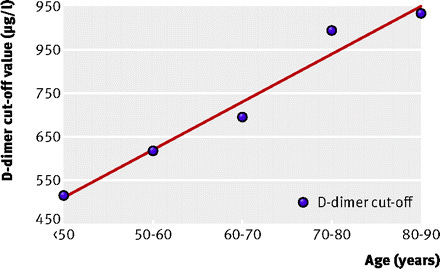
D-dimer tends to increase with age. To accommodate this known increase, while being able to reasonably rule out a pulmonary embolism suspicion, this BMJ article proposed an increasing cut-off of normal D-dimer by decade, as follows. [Note the likely typo where 950 is marked twice on the y-axis, instead of 950 and 850.]
Three of my five patients discussed above were still well above the cutoff for their (or any) age group by the BMJ criteria. Whereas the mean age of participants in the Italian study was 55, the mean age of participants in my study was 76.
Therefore, to account for this considerable age difference, I then assigned an age-based advantage to each of the five in the latter, subtracting 100 D-dimer points per decade (= 10 points per year) of age above 55, in accordance with the BMJ article calculations. That would render the age-adjusted table as follows, still significantly different than the Italian data:
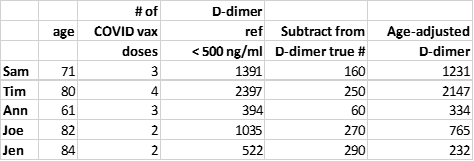
Adjusting for age still has all five of the US COVID-vaccinated subjects above the cutoff for optimal D-dimer < 221 from the Italian study. In contrast to the BMJ article, the large Italian study found no association of D-dimer levels with age.
Elevated D-dimer and COVID-vaccination
A new clinical syndrome, since February 2021, has been observed, vaccine-induced immune thrombotic thrombocytopenia (VITT), characterized by both clotting and low platelets. The two phenomena tend to have some opposing effects, because platelets are required in the clotting cascade, which is a 14-component process to create a barrier to bleeding, aka a clot.
In a case study, researchers had previously found significantly elevated D-dimer = 9050 mcg/L FEU = 9050 ng / mL = 18 x the top of the 500 ng / mL cut-off, in a patient with both thrombocytopenia and extensive venous thrombosis at one week following her COVID booster dose of the Pfizer-Biotech injection. Another VITT case presented 10 days after his second dose of Moderna vaccine with a D-dimer of 1890 ng/mL, and died 12 days after hospital admission. Another VITT patient had a D-dimer of 6.8 mg/L = 6800 ng/mL 20 days after a Moderna booster. Another (previously healthy) 76-year old VITT patient had D-dimer = 17,400 ng/mL at two days after his first Pfizer vaccine. His presentation to the hospital appeared as follows:

The American Society of Hematology limits criteria for diagnosis of VITT as being from 4 to 42 days post-COVID vaccine prior to symptom onset, along with presence of any venous or arterial thrombosis and thrombocytopenia with platelet count < 150 x 109/L, and markedly elevated D-dimer (>4 times upper limit of normal). These parameters would have excluded the above 76-year old unfortunate patient, who presented two days following his first Pfizer vaccine, although he met other criteria set by ASH.
The UK government’s Yellow Card system has reported “445 cases of major thromboembolic events (blood clots) with concurrent thrombocytopenia (low platelet counts) in the UK following vaccination with COVID-19 vaccine Astra Zeneca” mostly following the first dose, through November 23 2022. The same system found in that time period 33 such cases following the Pfizer vaccine and 8 cases following the Moderna vaccine.
There are contrarian perspectives however, as follows.
This observational study of 567 healthcare personnel denies any association between COVID vaccines and elevated D-dimer.
This article claims that VITT is “rare” following COVID vaccination, and perhaps it is.
However, each one of my COVID-vaccinated patients who agreed to be tested for D-Dimer were at 79th percentile (Ann) up to above (up to way above) normal range (Sam, Tim, Joe and Jen). All five were above the range found in 2013 southern Italy for optimal longevity (< 221). I would then have to question the suggestion that thrombogenic events associated with COVID-vaccination as being either non-existent or rare.
[This post is too long for e-mail, but you’re near the end of it. Please see the remainder of this article at colleenhuber.substack.com. . . . And here’s the rest.]
Diseases correlated with elevated D-dimer
D-dimer can be used, among other indicators, of cancer risk. In this study, very high D-dimer levels correlated with higher incidence of cancer:
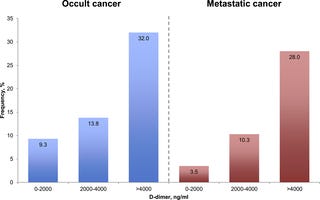
In the latter data, I have to note that both forward and reverse causality may be at work. That is, either a pro-coagulant effect of cancer, or a carcinogenic effect of thrombosis – or both – may be at work. And there have been studies that support both directions of causality.
Let’s not get wild, folks
Of the people who consulted me during or throughout COVID, I pretty much warned everyone around me - at least those who stood still long enough to hear me out - to please avoid these vaccines like the plague. Some whom I had not seen in years, and now regret their jabs, have expressed anger that I didn’t reach out to warn them. I did publish my dire warnings about the COVID vaccines above on February 21, 2021, before most Americans had taken the COVID shots, but I did not reach out individually to thousands of patients who have consulted with me over my 16 years of medical practice. My reply is that I also do not stand at the edge of each cliff with a sign that says:
Look, I just can’t be everywhere, advising everyone to quit playing Russian roulette, or to not take a stroll in the fast lane of a highway at night. There are only so many warnings I can broadcast, and those are with exceedingly small reach. Suffice it to say, let’s consult (either with me or with another contrarian, critical thinking or independent medical professional) before undertaking risky or experimental injections and other questionable practices.
This is shocking! Out of twelve patients who took the jab, one died a few days later and another had a return of a cancer that had been in remission for 5 years! Of the others who agreed to D-dimer test, all but one had elevated levels. The shots are damaging nearly everyone! And yet, the mass murder continues.... :-(
Extremely interesting post Dr Huber. It amazes me when I reflect on the medical training I have received in the last 3 years from people like yourself and many others. I sometimes pridefully think I just may know more about some of these things than most allopathic docs! Thanks so much for your tireless work.