


Heart fatigue from vaccines, as shown by fluid dynamics
Blowing water out of a straw is easy, right? What if it were milk instead? No problem. What if it were maple syrup? What if your heart were challenged to make a similar effort 24 / 7 ?

© Colleen Huber, NMD
The path of blood from the heart through the body’s circulatory system takes the liquid portion of blood, its cells and dissolved nutrients through a path from wide to narrow to wide again. This happens when the blood, pumped from the left ventricle of the heart, flows through the wide aorta (our body’s main central artery), and is then pushed through ever-narrower arteries. Then in turn, these branch into narrower arterioles, and finally into the capillaries. The capillaries are so small, so thin, that even a microscopic red blood cell must fold and momentarily deform a bit, in order to make it through that tunnel in order to get some elbow room, so to speak, on to a venule, then a vein, and then to the spacious vena cava (our body’s central vein) in its perpetual round trip journey back to the heart.
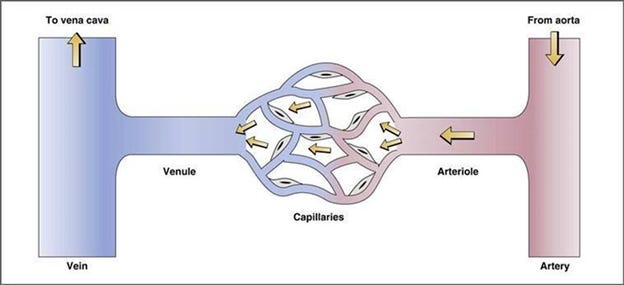
From Hemodynamics, Cardiovascular Physiology, Physiology, 5th ed.
When blood is normally thin, this journey has little resistance – even with narrowing vessels, because there are an increasing number of those vessels on roughly parallel paths, dividing the flow of blood. Blood pressure stays low to moderate, and the heart does not have to work particularly hard to move blood around.
But blood is not always thin these days. The cardiovascular effects of the COVID vaccines are comparable to placing many rocks in the creek, so to speak, which in an actual creek would change smooth flow to turbulence, stagnant eddies here, and rapids there.

The mRNA vaccines deliver an estimated 40 trillion packets of mRNA instruction code for human cells to produce spike proteins. The “spikes” are well-named, even while not jutting from coronaviruses, because when the spike proteins are released from the cells where they are produced, and then into the bloodstream and come to dock at the ACE-2 and CD-147 receptors, their position and shape disrupt the smooth surface of the inner lining, the endothelium, of the blood vessel.
Once laminar smooth flow of blood now becomes disrupted by turbulence and momentary stagnation, which immediately leads to clotting. But none of these are large injuries, so the phenomenon is a widespread micro-clotting and a general viscosity of blood. This illustration by Angeli and Spanevello, et al, shows spike protein production and release from cells to then float freely until the spike proteins dock onto the endothelial cells lining blood vessels and jut out into the lumen, just as boulders jut into the flowing water of a stream, changing the water’s motion. [1]
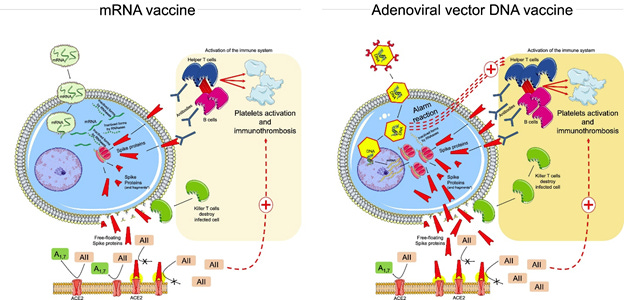
There are also CD-147 receptors and the effects of spike protein attachment there, as well as other considerations of endothelial cell death, inflammation associated with spike proteins, as well as the activity of platelets in the newly formed microclots. I discuss these mechanisms more elsewhere. [2]
How thick blood flows
As a stream of fluid (liquid or gas) is forced by the pumping of the heart against a constricted opening, both its speed (v) and kinetic energy (KE) increase. Bernoulli’s equation explains the physics principle of conservation of energy, in the specific case of a fluid being forced through a narrowed opening:

Where ρ is the fluid density, and the kinetic energy per unit volume KE/V is ½ of mass times the square of velocity (v) per total Volume (V). But don’t worry about that so much. More importantly, Bernoulli’s equation tells us that if there is something that raises the viscosity of blood, then there is a corresponding rise in the kinetic energy expended in moving blood around. According to Bernoulli’s equation above, the increased fluid density corresponds to a rise in energy used in moving blood through vessels. This would create more effort for the heart. We know from decades of experience with atherosclerotic patients, that when the heart labors to push blood through rigid blood vessels, then not only does blood pressure rise, but the overworked heart is at risk of congestive heart failure, which is a concerning disease that has a 30% survival rate a decade after diagnosis.
Resistance in the cardiovascular system is directly proportional to blood viscosity, where η is the viscosity of blood. (With a fluid, the tactile sensation of “viscosity” or thickness of a liquid, is quantified by osmolarity, often in mOsm/L. Osmolarity is just a quantifiable way of assessing viscosity.)
There is a further consideration with having viscous blood. The symbol π(c) represents capillary oncotic pressure, which means an inward pressure or the tendency to draw fluid inward. When π(c) increases, such as when blood is thickened by the involved process of conglomeration of various microclot components, then the plasma part of blood may tend to stay in the capillaries and not diffuse into the surrounding tissues. This would have the effect of increasing blood pressure, until other homeostatic mechanisms take effect.
Here is a corollary of Poiseuille’s equation, in which resistance (or the drudgery of pushing thick blood through the body) is proportional to the blood’s viscosity and to the length of the vessels, but is inversely related to the radius of the vessels.

So let’s say you got the COVID vaccine(s), but you still want to be able to have your heart push blood easily around your body. The above equation shows that resistance (R) increases when length (L) increases. This means that you have to blow water harder out through a very long straw than through a short straw. But resistance also increases when viscosity (η, pronounced EE-ta) increases. So you have more difficulty blowing maple syrup through a straw than water through a straw. The denominator of the equation gives a way out of the dilemma of COVID vaccine-induced viscosity creating extra resistance. The radius of the blood vessel is r. In Poiseuille’s equation, we see that r is in the denominator, so if the radius increases, then you can have lower resistance again. So vasodilation may be a strategy that clinicians explore if COVID vaccinated patients develop hypertension.
It’s possible that the problem of a chronically overworked heart could be medicated with positive inotropic agents, which boost heart pumping force, such as digoxin, but this risks pump burnout (heart failure) in the nearer term. So other strategies would include various ways to lower blood pressure by means of beta-blockers, ACE inhibitors and angiotensin receptor blocking drugs.
As an abundance of caution, it is important to not use any of the currently available COVID vaccines with either children or adults, until the cardiovascular consequences are better understood, or for those who are already vaccinated, to offer therapies that are appropriate for the cardiovascular consequences that patients present clinically.
[1] F Angeli, A Spanevello, et al. SARS-CoV-2 vaccines: Lights and shadows. Jun 1 2021. Eur J Int Med. Vol 88. P1-8.
https://www.ejinme.com/article/S0953-6205(21)00142-4/fulltext
[2] C Huber. Heart damage from the COVID vaccines: Is it avoidable? Jul 14 2021. PDMJ. https://pdmj.org/papers/myocarditis_paper
Am I right in thinking that. If this was any other drug or vaccine it would have been pulled from use?
Had covid 2 weeks ago. Took nothing for it. Felt bad about2-3 days. Aches and pains & low fever. On 4th day was about 85% normal. Slowly to 100% better. Have had far worse colds & flu. I am 67 Y.O. My wife had it worse than me but ok now.