


Root Canal Fillings and Their Effects
Three women at our clinic, each in their thirties, recently had interesting experiences with root canal filled teeth.

The first woman had four root canal filled teeth, had decided against keeping them, and then agreed with a dentist to extract four of them all at once, along with four impacted wisdom teeth. This was accompanied by discharge of profuse exudate (pus). Within hours afterward, the plantar fasciitis that she had suffered for years was gone. It later recurred, and then was relieved again after the tooth extraction site was further cleaned out. She also had had severe back pain for five years. That same night as the extraction of the eight teeth was the first night in five years that she could sleep horizontally without back pain. She had also had a melasma-type rash in each axilla (armpit). These both faded over the following weeks.
The second woman had been having rheumatoid arthritis symptoms for years. One of her two root canals had become painful, and her dentist extracted it. As soon as it was out of her mouth, the arthritic pain in her joints lessened considerably, and these symptoms, while still present to some extent, have been considerably less severe ever since that extraction. Some days there are no arthritic symptoms at all.
The third woman was driving a short commute while chewing gum, and the following item loosened, stuck to the chewing gum and simply fell out of her mouth.

And here is how that same tooth appeared earlier on x-ray.

This was tooth #30. That root canal was approximately 20 years old. It has not yet been replaced. After this happened, she experienced new onset palpitations, extreme sensitivity to sound and emotional lability for a whole day, which then went away. Nine months earlier, she had tooth #19, another root canal filled tooth, extracted. After the extraction, she felt immediate relief from sacral bone pain that she had had for the previous eight months. Then, the pain in the sacrum returned after the extracting site closed, and a jawbone cavitation was suspected.
Gutta percha filling material for root canals
Most root canals, if loosening and falling, would not be expected to look as in the above photo. The above tooth’s similar appearance to amalgam metal was surprising, to say the least. Gutta percha is the filling material of choice for root canal filling, and has been for decades.
Here is new gutta percha in its packaging:

Here is fresh gutta percha being placed:

There are photos that you can find on the internet of root canal teeth that have been extracted, which show gutta percha years after having been placed in the root canal of a tooth. Those photos may be somewhat unpleasant for readers. So instead of posting any of those, here is a one-minute video that the reader may choose to watch, or not, that shows extraction of a problematic root canal, and its white-yellowish (but blood-streaked) gutta percha root.

What all those videos and photos show is the light-color gutta percha material, and none show the metallic-appearing root that the driver found falling out of her mouth and into her lap. So the choice of filling material used in her case about 20 years ago was unusual to say the least.
Regarding filling material, a dental professional informed me that the gutta percha material that is used for root canal fillings has many times been seen to shrink back from the canal after placement, and that process is seen in the radiolucency that lines the canal at its apex on an older root canal filling. This process is often blamed on an endodontist not having bothered to fill the canal deeply enough. However, it is more likely that even with an endodontist’s diligent packing work, gutta percha shrinks back over time from the root apex, which may have to do with the chloroform that is used with it.
History of root canal association with chronic diseases
George Meinig, DDS wrote Root Canal Cover-Up in 1993. Although he had himself placed root canal fillings for many years, and had even co-founded the American Association of Endodontists (root canal therapists), he became increasingly wary of their effects on the rest of the body. Over time, Dr. Meinig’s observations of patients’ long-term experiences with their root canal fillings caused him concern, and he studied the prior work of Cleveland Ohio dentist Dr. Weston Price.
Dr. Price was a keen observer and a prolific writer on dental relationships to chronic diseases. He was one of the foremost health researchers of the 20th century. His classic 1938 book Nutrition and Physical Degeneration was the culmination of his interviews with people all over the world, both indigenous and migrant, land-based and urban.

Dr. Price wrote extensively, during a quarter century, of the vast range of diets and lifestyles and examined teeth of each of the people he interviewed. Within a single generation, an individual’s dietary choices showed strong correlation with development of the teeth. Price compared people of the same land and tribe, comparing those on their indigenous diet with those on a westernized diet. As it turned out, the western grain/sugar predominant diet did not have favorable outcomes on dental health for the people of any continent.
For example of the Seminole people in the Everglades forests of Florida, westernized diet was associated with a radically different dental configuration than those of the traditional Seminole diet: The photo on the left below is of a youth on the traditional Seminole diet, whereas the photo on the right is of a Seminole youth on a westernized diet.

On the remote Isle of Lewis, northwest of Scotland, the two brothers in the following photo had different diets. The younger brother, seen on the left, had years of a high-sugar diet, and rampant dental decay. The brother on the viewer’s right had maintained a traditional diet of seafood and oats.

Many more photos are in Dr. Price’s book, from his travels over a quarter century, from visits to the Maori people of New Zealand through Asia, Africa, Europe and the Americas.
Strep and other bacteria are sequestered in root canal filled teeth
When Dr. Price turned his attention to root canals, it began with his interest in his patients’ overall health conditions. One day, while treating the teeth of a woman confined to a wheelchair, with severe arthritis, he suspected that her root canal filling could possibly have harbored chronic infection, and he advised her to have it extracted, even though the tooth looked completely normal on x-rays.
The woman made a complete recovery from arthritis symptoms, no longer needing her wheelchair after this tooth was extracted, and was even able to do fine needlework again. However, Dr. Price implanted the extracted tooth under the skin of a rabbit. The rabbit did not fare well, developed crippling arthritis within 2 days, and then died in 10 days.
That experiment launched Price on an extensive series of experiments with extracted root canal teeth from humans, which he then implanted in rabbits, just under the skin. Every time he did this, not only did the rabbits each sicken and die within days, but the rabbits’ symptoms were the same as the human who had provided the tooth. Humans with kidney disease recovered, as the infected root canal tooth was extracted and then implanted into a rabbit, which then developed kidney disease. The same with liver disease, arthritis, cancer. Each time, the rabbit acquired the same or similar disease that the human had suffered from prior to extraction, and then each time the rabbit died 3 to 12 days later.
The overwhelming variety of the extracted teeth were found to have bacterial colonies, and most of those were Streptococcus.
Root canal filled teeth harbor so many bacteria for the following reasons.
First, gutta percha is a texturally ideal material to work with, for the objective of filling a narrow hole. However, it shrinks back over time, leaving a deep periapical space, which is seen on x-ray as radiolucency. Dr. Price wrote of this problem:
“When we consider how many thousands of the extracted teeth we have cultured and found to be infected within the tooth structure, and the extremely low percentage, practically zero, in which infection was not demonstrated, together with the fact that so many teeth with excellent root fillings show structural changes of the supporting tissues after a few years have elapsed, we are led to believe that root fillings rarely fill pulp canals sufficiently well to shut out bacteria completely. Root fillings usually fill the pulp canal much less some time after the operation, than at the time of the operation due to the contraction of the root canal filling material. The ultimate volume contraction of the root filling is approximately the amount of solvent used with gutta-percha as a root filling material.”
Second, each tooth contains three miles of microscopic tubules in the dentin layer, if all were attached together end-to-end. The tubules look like this under a scanning electron microscope, in cross-section and longitudinal views respectively:

Irrigation of the healthy tooth versus the root canal filled tooth
The fluid that flows through the dentinal tubules shown above is a transudate of extracellular fluid, containing electrolytes, minerals and proteins including albumin. Please note that the width of each tubule, about 2 microns, is far narrower than the diameter of a red blood cell, which is about 7-8 microns and the diameter of a macrophage, which is about 21 microns or a neutrophil at 12 microns or T and B cells at about 9 microns. So the cells in the blood cannot pass through the narrow dentinal tubules. While the cells of the immune system are also too large to pass through the tubules, the rinsing of water and electrolytes and such important immune system cytokines as interferons and interleukins still are small enough to flow through the tubules of a healthy tooth.

The healthy tooth above has the intact irrigation to have microbes and debris washed out of the tubules.
Contrast that unobstructed path of blood and extracellular fluid above with the root canal filled tooth below. When a root canal filling dams off the blood supply to the tooth, and the flow of dentinal fluid is now obstructed, and then stagnates, then colonies of microbes can no longer be moved through and washed away. Streptococcus bacteria are only 0.6 to 1.0 microns in diameter. So those can easily reside undisturbed and can multiply inside a tooth that has now lost its irrigation system, which had been connected to the flow of blood and lymph. The blockage occurs as in the root canal filled tooth diagram below.
The flow of dentinal fluid in an intact tooth is consistent with hydrodynamic principles, at a slight pressure of 1.47 kPa, and that flow likely is necessary to wash infection away from the tubules of a healthy tooth. Although it is not really known what happens to dentinal fluid after a root canal filling, it is likely that the fluid’s motion is now dammed by gutta percha blocking the flow of blood. Here is a diagram of a tooth undergoing a root canal filling:

In the lower diagram, the blood vessels are getting removed, and now the dentinal tubules have been cut off from the circulation. The root canal-filled tooth now cannot be rinsed of microbes that are just narrower than the tubule diameter. So Streptococcus, at 0.6 to 1.0 microns, can fit inside a 1 to 2 micron diameter tubule without fluid flowing through to wash these away. And it happens that Price found Streptococcus as the main microbe in the infections surrounding and inside of root canal filled teeth.
Here are some scanning electron microscope photos showing dentinal tubules chock full of bacilli and cocci, such as Streptococcus, Enterococcus, and other microbes.
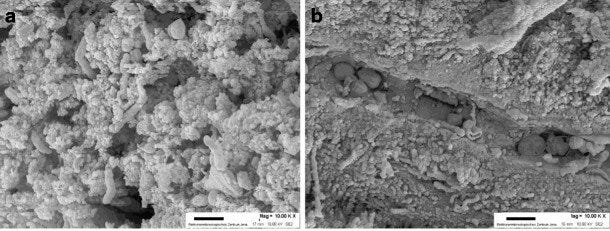
In the following photos the microbe Enterococcus faecalis has abundantly colonized dentinal tubules. Note the larger Candida albicans partially obstructing the tubules.

The authors of that study concluded that “Microorganisms can easily penetrate dentinal tubules of root canals with different appearance based on the microorganism size and dentinal tubules status.”
So now the problem becomes an intractable infection, which an antibiotic would have to travel three total miles to completely traverse all of the tubules in a tooth, a therapy unlikely to fully succeed.
Once a person’s last root-canal filled tooth is removed, then all of the areas of the body that might encounter microbes should now all be accessible to either the bloodstream or the immune system components carried in the extracellular fluid, in the case of the tubules of healthy teeth. So this may be why the people whose root canal fillings are extracted then recover from intractable, chronic disease, because now the immune system has access to the entire body, and bacteria no longer have anywhere to hide.
In a future article, I will discuss the extraordinary number of breast cancer patients at my clinic who have looked at a teeth meridians chart, such as this part of one here, and then let us know of their root canal fillings in teeth 20 or 21.

East Carolina University School of Dental Medicine says that 41,000 root canal fillings are placed every day in the US.
Perhaps it is time to re-think root canal fillings in dental treatment.
Dr. Huber, I am a dentist and thought I would respond to your interesting column.
First point: poorly done root canals are a hazard, not root canals in general. At a continuing education conference a few years ago, research was presented indicating that 50-60% of root canals done by general dentists failed while 90% performed by endodontists (root canal specialist) were successful. Skill matters a great deal in outcome of cases. Generally speaking (to keep this readable), it has been found that flushing the canal repeatedly and thoroughly with sodium hypochlorite was a big factor in outcome. Frankly, many general dentists rush through this process, while successful cases (and future referrals) are great practice builders for endodontists. As a general dentist, I would also say that discretion is the better part of endodontia (and oral surgery...). I refer anything that is beyond my skill level. In my experience, endodontists do a wonderful job with these difficult cases.
How do we know a root canal was done properly? Many times patients present with a large radiolucency apparent on the x-ray. If a root canal is done well, the radiolucency will completely resolve and stay resolved. The infection causing the radiolucency is eliminated.
The quick and the dirty: root canals, done well, are very effective. I would not hesitate to have one done.
An aside: the metallic "filling" attached to the crown in your story is a cast post, not a root canal filling.
If you have any question, please feel free to ask. Same for anyone on here.
I appreciate your work, Dr. Huber.
Just rinse up to 30 sec up to minutes with schwedenbitter* and add on 750ml 15 long-peppers to it....
*Make the schwedenbitter your self, the store version is lame. Get 2x 750ml grain alcohol 38% at +- 90 gr schwedenbitter mix to it leave it for at-least a month-6 weeks and if you can 3 months, filter it start rinsing...... Its yack, sharp etc.. You can also swallow the rinsing cause the herbs are great for everything else....., dilute it when swallowing with water....
Wanna know more get the maria treben books, they are translated is many languages.
https://www.amazon.com/Health-Through-Gods-Pharmacy-Experiences/dp/3850681246/ref=sr_1_5?crid=5904SPP5949E&keywords=Maria+treben&qid=1703878239&sprefix=maria+treben%2Caps%2C579&sr=8-5
https://www.amazon.de/-/en/Ihlich-Swedish-Bitters-Maria-Treben/dp/B0785J3TB9/ref=sr_1_6?crid=1VBUQG004T8OC&keywords=schwedenbitter+maria+treben+original&qid=1703878374&sprefix=schwedenbitter%2Caps%2C374&sr=8-6 you need the short one is about 15 herbs, that one works the best.
I personally added the long-pepper cause I had a huge infection under a molar with open filling, I put 15 long-peppers to 750ml already made schwedenbitter leave it warm for a month or a week under a halogen(heat) 20W lamp. It stings on the tongue, but I got every big root infection away for 6-7 years now.
I also have one root canal, but no longer infections around it due to the schwedenbitter rinsing. That's how I discovered it....
Enjoy!