

There was no pandemic in 2020
Deaths from all causes tell a truer story of a pandemic or lack thereof than a flawed and unstandardized testing method of a likely untestable virus. From Boris Borovoy's and my peer-reviewed paper

Abstract
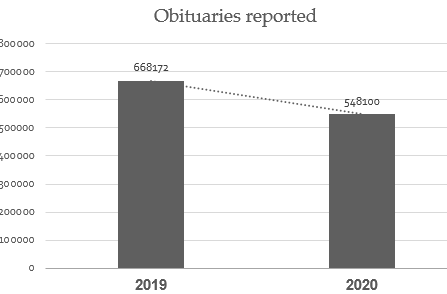
A pandemic that calls the attention of the public, and action by the medical field, is one that raises the total death rate above that of a typical year or season. The COVID-19 era that began in early 2020 has received continuous and rapt attention in the United States for deaths that have occurred. Has COVID-19 resulted in more deaths (known as “excess deaths”) than would have happened in a typical year? An obstacle to answering that question is that COVID-19 testing is flawed and imprecise, for reasons discussed herein, and it is difficult to distinguish COVID-19 from other respiratory illnesses, due to symptoms and signs that are mostly indistinguishable from the common cold, flu or pneumonia. It is possible that deaths of multiple causes have been ascribed to COVID-19, especially due to new peculiarities in mortality reporting during 2020 discussed herein. Therefore, year-over-year comparison of deaths from all causes is likely the best analysis of available evidence of whether the United States is now confronted by a deadly pandemic. The CDC mortality numbers are as yet unaudited by independent parties. Therefore, we compare numbers of obituaries in 2020 and 2019, which are verifiable reports of deaths of specific, identified individuals. We also examine the earnings statements of the largest medical suppliers in the US, to see if their sales of medical oxygen and other medical equipment prove a pandemic. These data all indicate that there has been no pandemic in the US in 2020.
Background
A pandemic is the prevalent spread of a disease over an entire country or worldwide, and there is often increased mortality for its duration compared to more typical years. Early rises in death rate are a warning of an especially dangerous pandemic. In 2020, it has been widely assumed that COVID-19 is an unusually deadly pandemic.
Understanding the COVID-19 phenomenon has been obstructed by several factors.
COVID-19 is assumed to be caused by a coronavirus that is said to be novel, “SARS-Cov-2.” However, SARS is likely a misnomer, because it is an abbreviation of Severe Acute Respiratory Syndrome. It is not at all clear that a majority or even a significant minority of COVID-19 patients have had acute respiratory distress with this illness. Other factors, such as use of over-pressurized ventilators, have led to acute respiratory distress among COVID-19 patients.
The most confusing aspect of COVID-19 is reliance on a manufacturing technique, now nearly universally re-purposed as a test for the presence of the SARS-Cov-2 virus, although there are many problems with this “test.” We list these problems below:
1. The very questionable applicability of the manufacturing technique, the reverse-transcriptase / polymerase chain reaction technique for propagating RNA, now used throughout the world as a test for presence of the particular infectious agent in question, or of other coronaviruses, virions and virus particles that may resemble or share common nucleic acid sequences with the SARS-Cov-2 infectious agent, without distinction among those; and
2. The 80% and higher false positive rate of this “test” in the diagnosis of COVID-19, partially due to cross-immunity to fragments of other coronaviruses, inevitably present in the human body, [i] [ii] followed by political pressure to recant these findings; and
3. The arbitrary number of iterations of this “test” (cycle thresholds) that must be selected to produce a positive “result”; and
4. Instructions given to physicians by the CDC to code cases as COVID-19 deaths including presumptively, even though multiple severe co-morbidities are typical among individuals whose deaths were called COVID-19; [iii] and
5. Controversy regarding higher Medicare and private insurance reimbursement for COVID-19 patients than for flu patients, [iv] [v] which may have skewed reported cause of death on death certificates; and
6. Generous financial rewards to hospitals by the US CARES Act for the number of COVID-19 patients they treat; and
7. The possibility that there may be political influences in altering the true number of deaths from COVID-19.
Two of these problems in particular merit greater attention.
COVID-19 has been very heavily marketed as a pandemic to the US public, with two important aspects that led to false reporting of US mortality data for COVID-19.
The incentive for mis-stated US mortality data is the financial influence created by the US CARES Act, which budgeted $175 billion dollars for distribution to hospitals for treatment of COVID-19 patients, with many hospitals receiving millions of dollars in such aid. [vi] Specific financial incentives that favored COVID-19 diagnosis over other similar diagnoses such as flu, pneumonia and bronchitis especially, included a Medicare incentive of only $5,000 per patient for pneumonia, but $13,000 per patient for the pathologically indistinguishable COVID-19 pneumonia. [vii] [viii] Further, the CARES Act incentive of $39,000 to treat such a patient with a ventilator resulted in financially lucrative outcomes for hospitals, but medically lethal outcomes for patients.[ix]
The core of public confusion and fear of COVID-19 stems from the testing itself. Reverse-transcriptase, polymerase chain reaction (RT-PCR) is a manufacturing technique for producing more RNA nucleic acid sequences. It was not intended by its inventor, the late Kary Mullis, PhD, as a test for an infectious disease. He warned against its use in such an application. He especially warned that it could be misused if the cycles, or iterations, of this procedure were processed too many times on a particular specimen. Regarding the use of RT-PCR to attempt to detect infectious disease, he said, at 35 or 40 cycles, “you can find almost anything in anybody.” [x] The CDC acknowledges that 33 cycles or more are unlikely to detect active virus. [xi] The number of cycles used in “COVID-19 testing” in the US have been above 37, and often well into the 40’s for all of 2020. [xii] [xiii] Laboratories in the US do not disclose the cycle thresholds that they use in running RT-PCR SARS-CoV-2 tests, except in Florida where the disclosure is mandatory. [xiv] No standardization for cycle threshold values exists across different tests and different laboratories.[xv]
Infectivity was found to be significantly reduced from positive tests when cycles were greater than 24, and that for every 1-unit increase in cycle threshold, the odds ratio of infectivity decreased by 32%. [xvi] Researchers concluded that PCR sensitivity is excellent (can find viral particles very easily), but that its specificity for detecting replicative (active) virus is poor, [xvii] as Dr. Mullis had warned. Nevertheless, RT-PCR has become “the COVID-19 test” used ubiquitously throughout the US and many other countries.
The magnitude of deception resulting from this misuse, overuse, over-cycling and over-advertising of PCR as a COVID-19 testing technique, along with frequent exhortations by politicians to “get tested,” can hardly be overstated. This is the core of the problem of the public falsely believing that there is a pandemic, and that its name is COVID-19.
Therefore, in order to attain the truest picture of the impact of the COVID-19 on public health, it would be helpful to look at deaths from all causes, to see if there has been a significant change.
Continued in Primary Doctor Medical Journal: https://pdmj.org/papers/is_there_a_pandemic/
References
[i] Y Zhou, Y Hou, et al. A network medicine approach to investigation and population-based validation of disease manifestations and drug repurposing for COVID-19. PLOS Biology. Nov 6 2020. https://journals.plos.org/plosbiology/article?id=10.1371/journal.pbio.3000970
[ii] G Zhuang, M Shen, et al. Potential false-positive rate among the ‘asymptomatic infected individuals’ in close contacts of COVID-19 patients.
[iii] US Health and Human Services, NVSS. Vital statistics reporting guidance. Apr 3, 2020.
[iv] M Rogers. Fact check: Hospitals get paid more if patients listed as COVID-19, on ventilators. USA Today. Apr 24, 2020. https://www.usatoday.com/story/news/factcheck/2020/04/24/fact-check-medicare-hospitals-paid-more-covid-19-patients-coronavirus/3000638001/
[v] K Waddill. Private payer COVID-19 reimbursement rates are twice Medicare rates. Health Payer Intelligence. Jul 13, 2020.
[vi] US Department of Health and Human Services. CARES Act Provider Relief Fund. HHS. https://www.hhs.gov/coronavirus/cares-act-provider-relief-fund/index.html
[vii] American Hospital Association. Special Bulletin: Senate passes the Coronavirus Aid, Relief and Economic Security (CARES) Act. https://www.aha.org/special-bulletin/2020-03-26-senate-passes-coronavirus-aid-relief-and-economic-security-cares-act
[viii] M Rogers. Fact check: Hospitals get paid more if patients listed as COVID-19, on ventilators. USA Today. Apr 24 2020. https://www.usatoday.com/story/news/factcheck/2020/04/24/fact-check-medicare-hospitals-paid-more-covid-19-patients-coronavirus/3000638001/
[ix] S Begley. With ventilators running out, doctors say the machines are overused for COVID-19. STAT. Apr 8 2020. https://www.statnews.com/2020/04/08/doctors-say-ventilators-overused-for-covid-19/
[x] K Mullis, interviewed. Every scary thing you’re being told depends on the unreliable PCR test. English Rose. Bitchute video. https://www.bitchute.com/video/UbKDEvIG6m2t/
[xi] US Centers for Disease Control and Prevention. Duration of isolation and precautions for adults with COVID-19. Oct 19 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/duration-isolation.html
[xii] M Landry. Your coronavirus test is positive. Maybe it shouldn’t be. Clinical Virology Laboratory, Yale New Haven Hospital. https://medicine.yale.edu/labmed/sections/virology/COVID-19%20Ct%20values_YNHH%20Aug.%202020%20_395430_36854_v1.pdf
[xiii] A Mandavilli. Your coronavirus test is positive. Maybe it shouldn’t be. New York Times. Aug 29 2020. https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
[xiv] Governor R DeSantis. Mandatory reporting of COVID-19 laboratory tests results: Reporting of cycle threshold values. Dec 3 2020. Florida Health. https://www.flhealthsource.gov/files/Laboratory-Reporting-CT-Values-12032020.pdf
[xv] AACC. SARS-CoV-2 cycle threshold: a metric that matters (or not). Dec 3 2020. American Association for Clinical Chemistry. https://www.aacc.org/cln/cln-stat/2020/december/3/sars-cov-2-cycle-threshold-a-metric-that-matters-or-not
[xvi] J Bullard, K Dust, et al. Predicting infectious severe acute respiratory syndrome coronavirus 2 from diagnostic samples. Clin Infect Dis. 71 (10). Nov 15 2020. https://academic.oup.com/cid/article/71/10/2663/5842165
[xvii] J Strong, H Feldmann. The crux of Ebola diagnostics. J Infect Dis. Dec 1 2017 (216). https://academic.oup.com/jid/article/216/11/1340/4210467
Your critics will call you a Covid denier but thank you for presenting the facts! Covid is being used both for political control and financial gain for sure. Half the people are waking up but it doesn’t seem like the woke will ever wake up?
Knowledge is the tool of the Masters. When Copernicus discovered that the Sun doesn't revolve around the Earth, it was a problem because it disturbed the narrative of the day. As we all know.
I don't think that the self proclaimed elite discuss wokeism, critical race theory or Covid-19 at their dinner table, other than as an instrument of control. I can imagine however that human ingenuity has brought us very far. And that from here on forward, in the face of overcrowding and resource depletion and with the help of artificial intelligence, a great reset could make sense if you belong to a class of stinking rich psychopaths.
The fact that Fauci is connected to Wuhan, that early treatment isn't allowed and that leading politicians in most of the Western civilisation has been schooled by the World Economic Forum tells me all I need to know in order to avoid the vax for now at least and instead focus on taking care of my health. On that note, I'm very glad I bought your book Colleen. It has taught me a lot. I take care of my diet, supplements and go out in nature on mountain trails where I live almost every day after work. Best regards from Norway!