


Prion Risks in the COVID Vaccines
Let's summarize the evidence to date linking the mRNA vaccines to prion-like protein mis-folding and consequent brain injury

Concerns have arisen about “mad cow” type disease, known as Creutzfeldt-Jakob disease (CJD), in humans exposed to the COVID vaccines. Those diseases are known as transmissible spongiform encephalopathies (TSE), the first in cows and the second in humans, and they are always fatal, generally within a few months to a year. German neurologists Creutzfeldt and Jakob were the first to describe such illness in the 1920s.
A macroscopic view
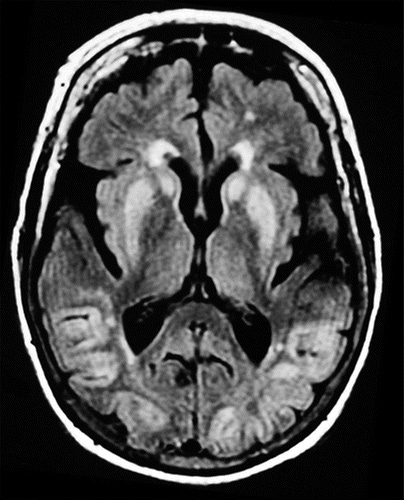
The word spongiform describes the devastation to a victim’s brain: a loss of solid mass that is seen on autopsy as shrinkage of gray matter. [1] The photo below shows that the brain has retracted from the skull, with large gaps and deep grooves, in a Creutzfeldt-Jakob victim. [2]
In contrast, here is a normal brain at about the same level as in the photo above, the normal one filling out the space to the skull more completely. [3]

A microscopic view
While there is a loss of so many neurons as to shrink or collapse the brain, there is also a notable loss microscopically. In the photo below, sponge-like holes open up brain tissue, as indicated by the yellow arrow, a process called vacuolation. [4]

A rapidly progressive dementia, muscle functional deficits, visual disturbances, convulsions and proprioception impairment are common hallmarks of CJD. [5] [6]
The medical literature prior to release of the COVID vaccines shows the most common routes of transmission to be iatrogenic, by tissue donation from a CJD victim, or contaminated, unsterilized surgical instruments [7] [8] or by injection of human growth hormone (hGH). [9] Mice that were inoculated with prion-containing material developed prion disease. [10]
TSE-type diseases are known as prion diseases. Prions are abnormally folded proteins, which are a kind of amyloid protein, which in themselves may not be such a threat. Some amyloids occur naturally throughout the body, and sperm could not swim without amyloid proteins. But CJD prions are especially dangerous, because they seem to trigger chain reaction production, in self-sustaining positive feedback, in which normal proteins then also transform to the abnormal prion proteins. With such a quickly multiplying effect, the brain is soon irreparably damaged. Disruption to neuronal cell function ensues, to the point of cell death.
A further difficulty is that prion proteins, like other amyloids, tend to lay flat against each other, more like neatly folded clothes in clean laundry, rather than clothes loosely piled into a washing machine. This dense folding makes the locked-inside component proteins unable to cross cell membranes or to otherwise interact normally with other proteins for needed cell functions.
Prions seem to be trafficked in envelopes called exosomes, [11] just as mRNA carried in lipid nanoparticles also travel, and the latter have been seen to travel with great efficiency. [12] This exosome transport is the likeliest means known so far of the rapid virulence of prion protein overwhelming the brain. The rapid spread of mRNA packets throughout the brain and the rest of the body was known by November 2020. [13]
SARS-CoV-2 proteins have been observed to interact with amyloidogenic proteins. [14] This is especially concerning given the self-perpetuating virulence with which prion-type proteins multiply. This induction of prion-like misfolding activity has also been seen with RNA-binding proteins, [15] and in the mRNA vaccines. [16] Seneff and Nigh show that the mRNA format of vaccines is highly risky for prion formation from the spike protein, affecting the vagus nerve initially before more widespread activity in the brain. [17] They show evidence that spike proteins generated by the mRNA vaccines build up toxic prion-like fibrils in neurons. [18]
After release of the COVID vaccines, in the year 2021 alone, there were over 200,000 reports of vagus-nerve related symptoms and signs that were linked to the COVID vaccines. That enormous number comprised over 97% of all cases with any such neurological symptoms, following any vaccine, in that year. [19]
With regard to COVID vaccines, the late Nobel laureate professor Luc Montagnier contributed to a paper published shortly before his death, in which 26 COVID-vaccinated individuals acquired the rare CJD so rapidly that 23 of the 26 developed symptoms of CJD within two weeks following their second dose of the mRNA COVID vaccine. Twenty of those CJD victims had already died by the time that paper was published, and those deaths occurred on average five months post-injection. [20] Then by June 2022, all six remaining patients had also died. The following graph shows the distribution of days from injection to first symptoms:

The researchers had also found that the CJD seen in these patients is more aggressive and quicker to progress than earlier forms of CJD.
I have cited Stephanie Seneff’s and Greg Nigh’s brilliant work extensively. Although the following list from one of the articles cited herein is only marginally relevant to the matter of prions, Seneff’s list below gives tremendous food for thought regarding the future risk-benefit considerations that would be prudent for individuals to make regarding injection of a brand-new product. [21]

Dr. Colleen Huber, author, Manifesto for a Cancer Patient, The Defeat of COVID and Neither Safe Nor Effective, The Evidence Against the COVID Vaccines, all on Amazon.
[1] D Manners, P Parchi, et al. Pathologic correlates of diffusion MRI changes in Creutzfeldt-Jakob disease. Apr 21 2009. Neurology. 72 (16). https://pubmed.ncbi.nlm.nih.gov/19380702/
[2] D Fragoso, A Lio da Mota, et al. Imaging of Creutzfeldt-Jakob disease: Imaging patterns and their differential diagnosis. Jan 11 2017. Radiographics. https://pubs.rsna.org/doi/abs/10.1148/rg.2017160075?journalCode=radiographics
[3] F Gaillard. Normal brain (MRI). https://radiopaedia.org/cases/normal-brain-mri-6
[4] G Dudhatra, A Kumar, et al. Transmissible spongiform encephalopathies affecting humans. Apr 2 2012. Hindawi. Intl Scholarly Res Notices. https://www.hindawi.com/journals/isrn/2013/387925/
[5] World Health Organization (WHO). Global surveillance, diagnosis and therapy of human transmissible spongiform encephalopathies: Report of a WHO consultation. Feb 9-11 1998. WHO. https://szu.cz/wp-content/uploads/2023/04/whoemczdi989.pdf
[6] H Lee, O Cohen, et al. Cerebral white matter disruption in Creutzfeldt-Jakob disease. Nov 2012. AJNR Am J Neuroradiol. 33 (10). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7964606/
[7] C Masters, J Harris, et al. Creutzfeldt-Jakob disease: patterns of worldwide occurrence and the significance of familial and sporadic clustering. 1979. Ann Neurology. 5 (2). 177-188. https://www.hindawi.com/journals/isrn/2013/387925/
[8] P Brown, M Preece, et al. Iatrogenic Creutzfeldt-Jakob disease at the millennium. 2000. Neurology. 55 (8). 1075-1081. https://www.hindawi.com/journals/isrn/2013/387925/
[9] P Brown, D Gajdusek, et al. Potential epidemic of Creutzfeldt-Jakob disease from human growth hormone therapy. 1985. NEJM. 313 (12) 728-731. https://www.nejm.org/doi/pdf/10.1056/NEJM198509193131205
[10] Y Eisele, U Obermuller, et al. Peripherally applied Abeta-containing inoculates induce cerebral beta-amyloidosis. Oct 21 2010. Europe PMC. 330 (6006). https://europepmc.org/article/MED/20966215
[11] I Porto-Carreiro, B Février, et al. Prions and exosomes: from PrPc trafficking to PrSc propagation. Sep-Oct 2005. Blood Cells Mol Dis. 35 (2). 143-148. https://pubmed.ncbi.nlm.nih.gov/16099696/
[12] M Maugeri, M Nawaz, et al. Linkage between endosomal escape of LNP-mRNA and loading into EVs for transport to other cells. Sep 24 2019. Nat Commun. 10 (4333). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6760118/
[13] Acuitas Therapeutics. Final Report: Test facility study No. 185350, Sponsor ref No. ALC-NC-0552. Nov 9 2020.
Appendix 2. https://phmpt.org/wp-content/uploads/2022/03/125742_S1_M4_4223_185350.pdf
[14] D Idrees, V Kumar. SARS-CoV-2 spike protein interactions with amyloidogenic proteins: Potential clues to neurodegeneration. May 21 2021. Biochem and Biophys Res Comm. 554. 94-98. https://www.sciencedirect.com/science/article/pii/S0006291X2100499X?via%3Dihub
[15] O King, A Gitler, et al. The tip of the iceberg: RNA-binding proteins with prion-like domains in neurodegenerative disease. Jun 26 2012. Brain Res. 1462: 61-80. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3372647/
[16] B Classen. COVID-19 RNA based vaccines and the risk of prion disease. Dec 27 2020. Microbiol & Inf Dis. https://scivisionpub.com/pdfs/covid19-rna-based-vaccines-and-the-risk-of-prion-disease-1503.pdf
[17] S Seneff, G Nigh. Worse than the disease? Reviewing some possible unintended consequences of the mRNA against COVID-19. May 10 2021. Intl J Vaccine Theory Practice Res. 2 (1). 38-79. https://dpbh.nv.gov/uploadedFiles/dpbhnvgov/content/Boards/BOH/Meetings/2021/SENEFF~1.PDF
[18] S Seneff, A Kyriakopoulos, et al. A potential role of the spike protein in neurodegenerative diseases: A narrative review. Feb 11 2023. Cureus. 15 (2). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9922164/
[19] S Seneff, G Nigh, et al. Innate immune suppression by SARS-CoV-2 mRNA vaccinations: The role of G-quadruplexes, exosomes and microRNAs. Jun 2022. Food Chem Toxicol. 164. 113008. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9012513/
[20] J Perez, C Moret-Chalmin, RIP Luc Montagnier. Towards the emergence of a new form of the neurodegenerative Creutzfeldt-Jakob disease: Twenty six cases of CJD declared a few days after a COVID-19 “vaccine” jab. Jun 14 2022. https://zenodo.org/record/6641999#.ZGP0HKXMJhE
Reprinted 2023 in Intl J Vaccine Theory, Practice Res. 3 (1). https://ijvtpr.com/index.php/IJVTPR/article/view/66
[21] S Seneff, G Nigh. Worse than the disease? Reviewing some possible unintended consequences of the mRNA against COVID-19. May 10 2021. Intl J Vaccine Theory Practice Res. 2 (1). 38-79. https://dpbh.nv.gov/uploadedFiles/dpbhnvgov/content/Boards/BOH/Meetings/2021/SENEFF~1.PDF
I read the paper by Seneff and Nigh just as my employer, my union, and my colleagues were settling on the grand idea that forcing everyone in the workplace to take the "safe and effective" shots was just the ticket for getting back to normal. I brought that article and many others to my boss who likely didn't even try to read it. Not an easy read for non-medical, non-scientists. Instead he said they had to defer to their "gold standard" docs at the prestigious and highly regarded hospital system here...which also happened to be the first in the country to mandate the injection. So "normal" looks like this...dozens of jabbed employees missing work during 2022 when Omicron continually reinfected them, 2 serious cases of cancer occuring in temporal proximity to the shot, a case of tremors made much worse, a case of autoimmune reaction and neuropathy which left a colleague completely unable to function in their job, a colleague battling serious and inexplicable rashes and hives unable to work, a colleague with frightening chest pains following their latest safe and effective booster, a recent retiree getting physical therapy for what appears to be a stroke, and another friend in the same field of work but employed elsewhere who spent the holidays hospitalized for blood clots.
I have also wondered if the increased risk for amyloid production described in Seneff's paper might have any relation to the amyloid like blockages embalmers are pulling from the deceased.
Three cheers for getting back to "normal". What have we done?
That graphic from the Seneff and Nigh paper gives me chills, when I think about the hysterical rush of the general population to inject themselves multiple times with this novel snake oil. Inject in haste, repent at leisure.